Coronary CT angiography (CCTA) identifies underlying heart disease in firefighters, who are at high occupational cardiovascular risk, according to research presented at the Society of Cardiovascular Computed Tomography (SCCT) meeting.
The findings underscore the need to screen at-risk populations beyond traditional tests, said Carrie Burns, MD, district physician for South Metro Fire Rescue in Centennial, CO, in a presentation delivered July 19. Burns' and colleagues' work received an SCCT Best Abstract Award.
"[We found that] implementation of screening CCTA … identified underlying CAD [coronary artery disease] in a large proportion of firefighters who were not identified at elevated cardiovascular risk by [traditional tests] and led to significant changes in preventive management," they wrote.
Sudden cardiac death is a leading cause of line-of-duty deaths in firefighters, accounting for 40% of duty-related firefighter deaths in 2023, Barnes explained. Among firefighters who die of sudden cardiac death, 80% had evidence of significant coronary artery disease, she said. But they may not be getting the screening they need.
"Firefighters are strong people with strong opinions," Barnes noted. "In general, they are adverse to medical evaluation, because like military personnel, police, and aviators, an evaluation could equal a condition that could make them non-operational for a time or lead to job loss."
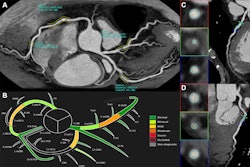
To address the need for more CAD screening among firefighters, Burns and colleagues created a program that screened for the condition using coronary CCTA with a technique called advanced quantitative coronary plaque analysis. Their hypothesis was that, by using this particular type of CT imaging with asymptomatic firefighters to screen for subclinical atherosclerotic cardiovascular disease (ASCVD), CAD could be diagnosed early and treatment strategies put into place.
The team conducted CCTA exams in 309 firefighters as part of a yearly occupational physical. All individuals aged 40 years or older or those with a cardiovascular risk factor were eligible for CCTA. Burns' group measured each person's cardiovascular risk factors and A1C, and calculated an American Heart Association's Predicting Risk of cardiovascular disease EVENTs (PREVENT) risk score. Study participants also underwent coronary artery calcium (CAC) scoring; the team measured quantitative coronary plaque analysis and stenosis using commercially available, AI-enabled software (Cleerly Labs).
The group found the following:
- 34% of firefighters had CAC scores over 0 (median score, 35).
- 88% had any coronary artery disease identified on CCTA.
- 83% of those with CAC scores equal to zero had noncalcified plaque.
- 9.1% of study participants had severe coronary artery disease burden identified by quantitative coronary plaque analysis on CCTA.
- 90.2% of firefighters with coronary plaque had nonobstructive coronary artery disease.
- 28.6% of firefighters were referred to cardiology for further lipid management based on quantitative coronary plaque findings.
The AHA PREVENT score did not identify patients with coronary artery disease on CCTA, Barnes explained.
"PREVENT scores frequently underestimate risk in this population and may result in delayed prevention strategies," she said.
The team is continuing the screening initiative and is gathering one-year follow-up data from last year, Barnes concluded, although she did note that there are challenges to the program, including the cost of the exams and managing participants' radiation exposure and any incidental findings.