Does the addition of plaque burden grade information improve Coronary Artery Disease-Reporting and Data System (CAD-RADS) scoring on coronary CT angiography (CCTA)? Perhaps not, researchers have reported.
The study results may help clarify when to use coronary artery calcium (CAC) scoring -- and thus could spare patients unnecessary radiation exposure, wrote a team led by Ji Won Lee, MD, PhD, of Pusan National University School of Medicine and Medical Research Institute in Busan, Korea. The group's work was published July 9 in the American Journal of Roentgenology.
"Given [our] present findings, the inclusion of an additional noncontrast acquisition for CAC scoring (with associated increased radiation exposure) within [CCTA] protocols may not improve risk stratification for patients presenting to the emergency department with acute chest pain," the investigators explained. "Nonetheless, CAC scoring may be useful for risk stratification in asymptomatic or low-risk patients who do not undergo contrast-enhanced [CCTA]."
CAD-RADS was launched in 2016, and its latest upgrade was released in 2022. It is now called CAD-RADS 2.0 and incorporates reporting of plaque burden grades via CAC scores in addition to stenosis categories in the following framework:
- 0 (0% stenosis and no plaque)
- 1 (1% to 24% stenosis or plaque with positive remodeling but no stenosis)
- 2 (25% to 49% mild stenosis)
- 3 (50% to 69% moderate stenosis)
- 4A (70% to 99% severe stenosis in 1 or 2 vessels)
- 4B (70% to 99% severe stenosis in 3 vessels or left main ≥50%)
- 5 (any 100% stenosis or total occlusion)
Lee and colleagues assessed the usefulness of plaque burden grades used with CAD-RADS categories for predicting cardiac events in patients presenting in the emergency department with acute chest pain. Their study included 2,032 patients who underwent CCTA in the emergency department at one of four centers between January 2018 to December 2021; they tested various combinations of different models/characteristics (Cox, C-statistic, clinical variables, plaque burden grades, CAD-RADS categories, and presence of high-risk plaque).
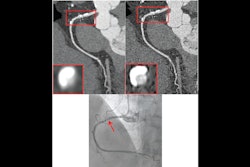
A single radiologist at each center reviewed exams and assigned a plaque burden grade by calculating a CAC score on noncontrast CT images, as well as a CAD-RADS category by assessing vessel stenosis on contrast-enhanced CTA images (both of these assessments were performed using CAD-RADS 2.0). Each of these radiologists also evaluated the exams for high-risk plaque. Finally, these radiologists reviewed each center's electronic medical record for cardiac events (composite outcome of cardiac-related death, myocardial infarction, or hospitalization for unstable angina).
During a median follow-up period of 15 months, 63 (3.1%) of patients experienced cardiac events, the group noted. It then reported the following:
- In a multivariable Cox model, cardiac events showed significant independent associations with CAD-RADS 3 (hazard ratio [HR] = 7.1, with 1 as reference), CAD-RADS 4 (HR = 13.6), CAD-RADS 5 (HR = 17.6), and high-risk plaque (HR = 2.5), but not with plaque burden grades.
- For predicting cardiac events, the C-statistic was 0.67 for a model that included clinical variables; 0.74 for a model that included clinical variables and plaque burden grades; 0.86 for a model that included clinical variables, CAD-RADS categories, and high-risk plaque; and 0.87 for a model that included clinical variables, plaque burden grades, CAD-RADS categories, and high-risk plaque.
- The model with clinical variables, CAD-RADS categories, and high-risk plaque, but without plaque burden grades, showed the highest net clinical benefit from 20% to 100%.
"CAD-RADS categories and the presence of high-risk plaque, assessed on coronary CTA, provided incremental prognostic utility over clinical variables in predicting cardiac events in patients presenting to the [emergency department] with chest pain," the investigators concluded.
The complete study can be found here.