Photon-counting detector CT (PCCT) offers improved coronary stent imaging over traditional CT by providing enhanced spatial resolution and spectral capabilities, according to a literature review published May 29 in Radiology: Cardiothoracic Imaging.
These "advancements of [PCCT] offer potential benefits to clinical care by enhancing the diagnostic accuracy of CT technology for assessing metallic stents, potentially diminishing the need for invasive procedures," wrote a team led by Judith van der Bie of Erasmus University Medical Center in Rotterdam, the Netherlands.
Using metallic stents is common for managing acute and chronic coronary artery disease, the group wrote. But the investigators also noted that re-narrowing of the artery (i.e., restenosis) caused by plaque or scar tissue is a major complication of this intervention. While invasive coronary angiography is the reference standard for assessing stents, use of noninvasive coronary CT angiography (CCTA) has increased. The problem is that assessing stent efficacy is impacted by stent diameter and limitations in resolution and high-density artifacts such as blooming artifacts of the stent and any surrounding calcifications, and CCTA has a low sensitivity range for imaging stents of 27% to 79% (although it has a specificity of 81% to 97%).
Van der Bie and colleagues conducted a literature review to explore whether PCCT's high spatial resolution reduces stent blooming artifacts and boosts in-stent visibility and restenosis assessment. They included 23 studies found on Embase, Medline, Web of Science, Cochrane, and Google Scholar databases through April 2024.
Overall, the group reported that the studies included in the review found that using PCCT for coronary stent imaging reduces blooming artifacts from stent struts and any adjacent calcifications, which translates to improved in-stent lumen visibility. The studies also stressed the importance of using thin sections and sharp kernels (the latter being algorithms that affect image sharpness and noise levels) for effective PCCT imaging of stents. Yet because these techniques tend to increase image noise -- which can negatively impact qualitative assessment of the lumen -- the use of higher strengths of iterative reconstruction algorithms is key.
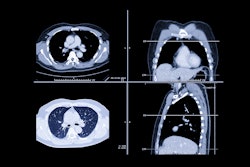
 Images in a 62-year-old male patient with a history of anteroseptal infarction, treated with percutaneous coronary intervention with stent placement in the left anterior descending artery (LAD) and right coronary artery (RCA), who presented with recurrent typical angina. The patient was scanned with a NAEOTOM Alpha photon-counting detector (PCD) CT system with contrast enhancement and an average heart rate of 57 beats per minute (140 kV, 0.2-mm section thickness, Bv56 kernel, iterative reconstruction strength of 4). (A) Multiplanar reformation image: The stent in the proximal RCA was occluded (lower arrow). The upper arrow indicates a significant stenosis. (B) Multiplanar reformation: Stent in the distal LAD appears patent (lower arrow), but a nonsignificant hypoattenuating region in the mid LAD was observed with PCD CT (middle arrow). Additionally, calcifications were observed at the origin of the first diagonal with a significant stenosis (upper arrow). (C) Invasive coronary angiographic image of the RCA helps confirm results found at PCD CT. The arrow indicates the occlusion of the RCA. (D) Invasive coronary angiographic image of the LAD helps confirm results found at PCD CT. Left arrow shows the nonsignificant stenosis in the mid LAD while the right arrow indicates the significant stenosis in the first diagonal. (E) Volume-rendered image of the heart. Images and caption courtesy of the RSNA.
Images in a 62-year-old male patient with a history of anteroseptal infarction, treated with percutaneous coronary intervention with stent placement in the left anterior descending artery (LAD) and right coronary artery (RCA), who presented with recurrent typical angina. The patient was scanned with a NAEOTOM Alpha photon-counting detector (PCD) CT system with contrast enhancement and an average heart rate of 57 beats per minute (140 kV, 0.2-mm section thickness, Bv56 kernel, iterative reconstruction strength of 4). (A) Multiplanar reformation image: The stent in the proximal RCA was occluded (lower arrow). The upper arrow indicates a significant stenosis. (B) Multiplanar reformation: Stent in the distal LAD appears patent (lower arrow), but a nonsignificant hypoattenuating region in the mid LAD was observed with PCD CT (middle arrow). Additionally, calcifications were observed at the origin of the first diagonal with a significant stenosis (upper arrow). (C) Invasive coronary angiographic image of the RCA helps confirm results found at PCD CT. The arrow indicates the occlusion of the RCA. (D) Invasive coronary angiographic image of the LAD helps confirm results found at PCD CT. Left arrow shows the nonsignificant stenosis in the mid LAD while the right arrow indicates the significant stenosis in the first diagonal. (E) Volume-rendered image of the heart. Images and caption courtesy of the RSNA.
"Beyond denoising algorithms, reducing noise in HR data can also be achieved by reconstructing [ultrahigh resolution] data into standard voxel sizes," the team wrote.
In any case, the team concluded that "the improved diagnostic accuracy of [PCCT] in the assessment of in-stent restenosis is promising for clinical patient care."
The complete study can be found here.